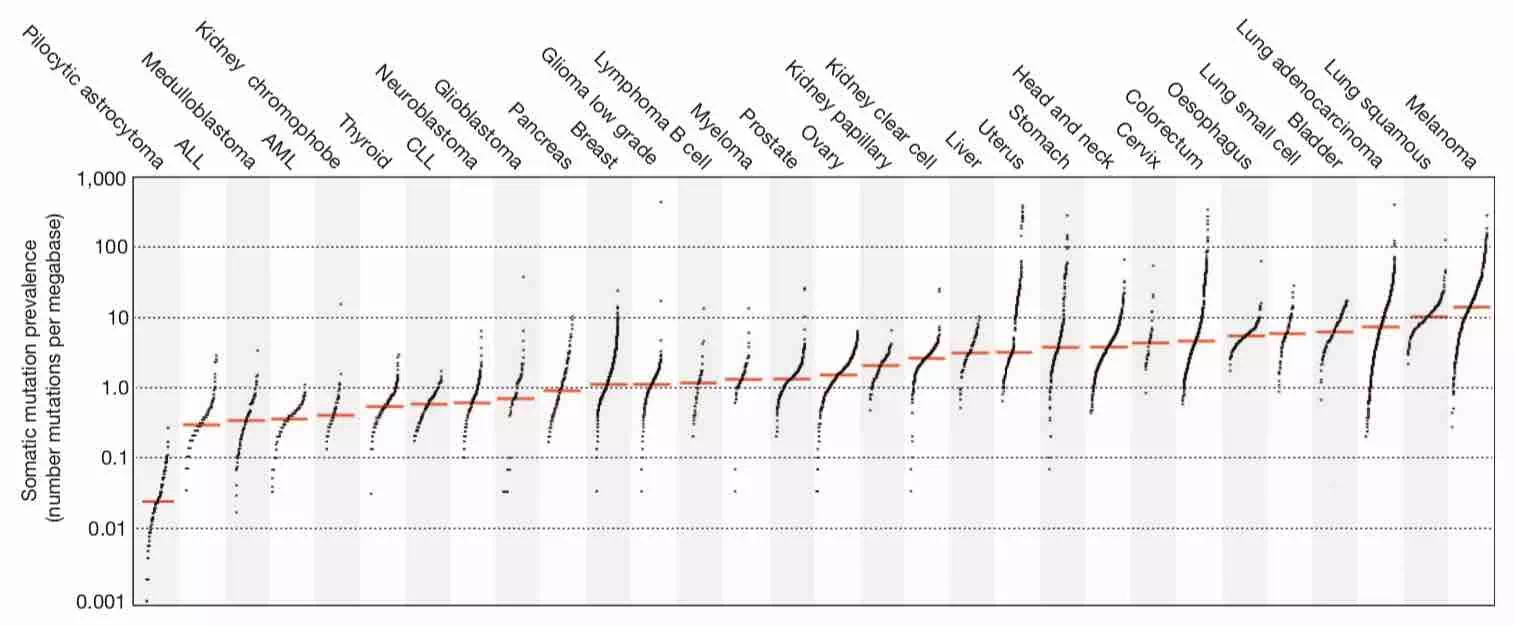
An analysis of mutations from over 7,000 cancers of diverse origins reveals the diversity of mutational processes underlying the development of cancer; more than 20 distinct mutational signatures are described, some of which are present in many cancer types, notably a signature attributed to the APOBEC family of cytidine deaminases, whereas others are specific to individual tumour types.
A large-scale analysis of hypermutation in human cancers provides insights into tumor
evolution dynamics and identifies clinically actionable mutation signatures.
MSK-IMPACT is a clinical sequencing platform able to detect genomic mutations, copy number alterations and structural variants in a panel of cancer-related genes. This assay is implemented prospectively to inform patient enrollment in genomically matched clinical trials at Memorial Sloan Kettering Cancer Center (MSKCC). Sequencing results of tumor and matched normal tissue from a cohort of >10,000 patients with detailed clinical annotation provide an overview of the genomic landscape of advanced solid cancers and bring new insights into molecularly guided cancer therapy.
PURPOSE Tumor mutational burden (TMB) is a developing biomarker in non–small-cell lung cancer (NSCLC). Little is known regarding differences between TMB and sample location, histology, or other biomarkers. METHODS A total of 3,424 unmatched NSCLC samples, including 2,351 lung adenocarcinomas (LUADs) and 1,073 lung squamous cell carcinomas (LUSCs), underwent profiling, including next-generation sequencing of 592 cancer-related genes, programmed death ligand 1 immunohistochemistry, and TMB. The rate TMB of 10 mutations per megabase (Mb) or greater was compared between primary and metastatic LUAD and LUSC. Molecular alteration frequency was compared at a cutoff of 10 mutations/Mb. RESULTS LUAD metastases were more likely to have a TMB of 10 mutations/Mb or greater compared with primary LUADs (38% v 25%; P < .001), and this difference was most pronounced with brain metastases (61% v 35% for other metastases; P < .001). The median TMB for LUAD brain metastases was 13 mutations/Mb compared with six mutations/Mb for primary LUADs. Variability existed for other LUAD metastasis sites, with adrenal metastases most likely to meet the cutoff of 10 mutations/Mb (51%) and bone metastases least likely to meet the cutoff (19%). TMB was more commonly 10 mutations/Mb or greater for LUSC primary tumors than for LUAD primary tumors (35% v 25%, respectively; P < .001). LUSC metastases were more likely to have a TMB of 10 mutations/Mb or greater than LUSC primary tumors. Poorly differentiated disease was more likely have a TMB of 10 mutations/Mb or greater when stratified by histology and primary tumor or metastasis. Site-specific molecular differences existed at this TMB cutoff including programmed death ligand 1 positivity and STK11 and KRAS mutation rate. CONCLUSION TMB is a site-specific biomarker in NSCLC with important spatial and histologic differences. TMB is more frequently 10 mutations/Mb or greater in LUAD and LUSC metastases and highest in LUAD brain metastases. Along this TMB cutoff, clinically informative distinctions exist in other tumor profiling characteristics. Further investigation is needed to expand on these findings.
Cancer Research UK, UK National Institute for Health Research (NIHR) at the Royal Marsden Hospital National Health Service Foundation Trust, Institute of Cancer Research and University College London Hospitals Biomedical Research Centres, the UK Medical Research Council, the Rosetrees Trust, Novo No …
These results show that a CGP assay targeting ~1.1 Mb of coding genome can accurately assess TMB compared with sequencing the whole exome. Using this method, we find that many disease types have a substantial portion of patients with high TMB who might benefit from immunotherapy. Finally, we identif …
Cancers with a defective DNA mismatch repair (dMMR) system contain thousands of mutations
most frequently located in monomorphic microsatellites and are thereby defined as
having microsatellite instability (MSI). Therefore, MSI is a marker of dMMR. MSI/dMMR
can be identified using immunohistochemistry to detect loss of MMR proteins and/or
molecular tests to show microsatellite alterations. Together with tumour mutational
burden (TMB) and PD-1/PD-L1 expression, it plays a role as a predictive biomarker
for immunotherapy.
We present an extensive assessment of mutation burden through sequencing analysis of >81,000 tumors from pediatric and adult patients, including tumors with hypermutation caused by chemotherapy, carcinogens, or germline alterations. Hypermutation was detected in tumor types not previously associa …
High mutational loads are associated with improved survival in melanoma patients but
are not predictive of response to anti-PD-1 therapy, suggesting that other genomic
and non-genomic features also contribute to response patterns on PD-1 checkpoint blockade
therapy.
Immune checkpoint inhibitors, which unleash a patient’s own T cells to kill tumors, are revolutionizing cancer treatment. To unravel the genomic determinants of response to this therapy, we used whole-exome sequencing of non–small cell lung cancers treated with pembrolizumab, an antibody targeting programmed cell death-1 (PD-1). In two independent cohorts, higher nonsynonymous mutation burden in tumors was associated with improved objective response, durable clinical benefit, and progression-free survival. Efficacy also correlated with the molecular smoking signature, higher neoantigen burden, and DNA repair pathway mutations; each factor was also associated with mutation burden. In one responder, neoantigen-specific CD8+ T cell responses paralleled tumor regression, suggesting that anti–PD-1 therapy enhances neoantigen-specific T cell reactivity. Our results suggest that the genomic landscape of lung cancers shapes response to anti–PD-1 therapy.
Despite the remarkable success of cancer immunotherapies, many patients do not respond to treatment. Rizvi et al. studied the tumors of patients with non–small-cell lung cancer undergoing immunotherapy. In two independent cohorts, treatment efficacy was associated with a higher number of mutations in the tumors. In one patient, a tumor-specific T cell response paralleled tumor regression.
Science , this issue p. [124][1]
[1]: /lookup/doi/10.1126/science.aaa1348
Hellmann et al. examine non-small-cell lung cancers treated with combined PD-1 and
CTLA-4 blockade using whole-exome sequencing and find that high tumor mutation burden
is the strongest feature associated with improved objective response, durable benefit,
and progression-free survival in multivariable analysis.
Hellmann et al. evaluate the impact of tumor mutational burden on the efficacy of
nivolumab monotherapy or combination with ipilimumab in patients with small-cell lung
cancer (SCLC). They show that treatment efficacy and the increased benefit of the
combination are most substantial in SCLC with high tumor mutational burden.
Atezolizumab showed durable activity and good tolerability in this patient population.
Increased levels of PD-L1 expression on immune cells were associated with increased
response. This report is the first to show the association of TCGA subtypes with response
to immune checkpoint inhibition and to show the importance of mutation load as a biomarker
of response to this class of agents in advanced urothelial carcinoma.
Atezolizumab showed durable activity and good tolerability in this patient population.
Increased levels of PD-L1 expression on immune cells were associated with increased
response. This report is the first to show the association of TCGA subtypes with response
to immune checkpoint inhibition and to show the importance of mutation load as a biomarker
of response to this class of agents in advanced urothelial carcinoma.
Treatment with immune checkpoint blockade (ICB) with agents such as anti-programmed cell death protein 1 (PD-1), anti-programmed death-ligand 1 (PD-L1), and/or anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) can result in impressive response ...
Immunologic checkpoint blockade with antibodies that target cytotoxic T lymphocyte–associated antigen 4 (CTLA-4) and the programmed cell death protein 1 pathway (PD-1/PD-L1) have demonstrated promise in a variety of malignancies. Ipilimumab (CTLA-4) and pembrolizumab (PD-1) are approved by the US Food and Drug Administration for the treatment of advanced melanoma, and additional regulatory approvals are expected across the oncologic spectrum for a variety of other agents that target these pathways. Treatment with both CTLA-4 and PD-1/PD-L1 blockade is associated with a unique pattern of adverse events called immune-related adverse events, and occasionally, unusual kinetics of tumor response are seen. Combination approaches involving CTLA-4 and PD-1/PD-L1 blockade are being investigated to determine whether they enhance the efficacy of either approach alone. Principles learned during the development of CTLA-4 and PD-1/PD-L1 approaches will likely be used as new immunologic checkpoint blocking antibodies begin clinical investigation.
The mechanisms by which immune checkpoint blockade modulates tumor evolution during therapy are unclear. We assessed genomic changes in tumors from 68 patients with advanced melanoma, who progressed on ipilimumab or were ipilimumab-naive, before and after nivolumab initiation (CA209-038 study). Tumo …
Analysis of advanced cancer patients treated with immune-checkpoint inhibitors shows that tumor mutational burden, as assessed by targeted next-generation sequencing, predicts survival after immunotherapy across multiple cancer types.
PURPOSE Genomes of tumors that are deficient in DNA mismatch repair (dMMR) have high microsatellite instability (MSI-H) and harbor hundreds to thousands of somatic mutations that encode potential neoantigens. Such tumors are therefore likely to be immunogenic, triggering upregulation of immune checkpoint proteins. Pembrolizumab, an anti‒programmed death-1 monoclonal antibody, has antitumor activity against MSI-H/dMMR cancer. We report data from the phase II KEYNOTE-158 study of pembrolizumab in patients with previously treated, advanced noncolorectal MSI-H/dMMR cancer. PATIENTS AND METHODS Eligible patients with histologically/cytologically confirmed MSI-H/dMMR advanced noncolorectal cancer who experienced failure with prior therapy received pembrolizumab 200 mg once every 3 weeks for 2 years or until disease progression, unacceptable toxicity, or patient withdrawal. Radiologic imaging was performed every 9 weeks for the first year of therapy and every 12 weeks thereafter. The primary end point was objective response rate per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, as assessed by independent central radiologic review. RESULTS Among 233 enrolled patients, 27 tumor types were represented, with endometrial, gastric, cholangiocarcinoma, and pancreatic cancers being the most common. Median follow up was 13.4 months. Objective response rate was 34.3% (95% CI, 28.3% to 40.8%). Median progression-free survival was 4.1 months (95% CI, 2.4 to 4.9 months) and median overall survival was 23.5 months (95% CI, 13.5 months to not reached). Treatment-related adverse events occurred in 151 patients (64.8%). Thirty-four patients (14.6%) had grade 3 to 5 treatment-related adverse events. Grade 5 pneumonia occurred in one patient; there were no other treatment-related fatal adverse events. CONCLUSION Our study demonstrates the clinical benefit of anti–programmed death-1 therapy with pembrolizumab among patients with previously treated unresectable or metastatic MSI-H/dMMR noncolorectal cancer. Toxicity was consistent with previous experience of pembrolizumab monotherapy.